A 64-year-old female life-long nonsmoker was referred for spirometry testing because of increasing cough, wheezing, and exercise intolerance. The patient had been previously diagnosed with asthma and took albuterol as needed (monotherapy). Pre-bronchodilator spirometry revealed moderately severe obstruction.

Figure 1. Pre-bronchodilator spirometry data
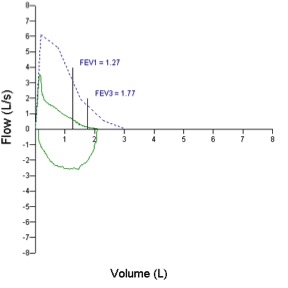
Figure 2. Pre-bronchodilator flow-volume loop.
The patient was given an updraft nebulizer treatment with 2.5 mg albuterol and 0.5 mg ipratropium.
Post bronchodilator spirometry testing revealed an extraordinary increase in airflow.
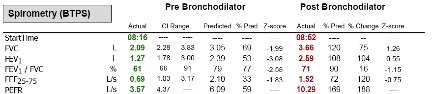
Figure 3. Pre and post-bronchodilator data.
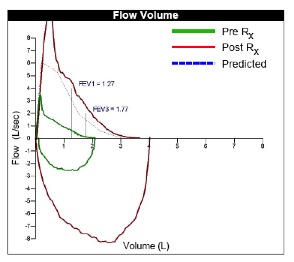
Figure 4. Pre and post flow-volume loops
The technologist was skeptical of this apparent normalization of pulmonary function due to the supra-normal peak flow rate (10.29 L/s, 169% predicted).
Inspection of the pressure differential pneumotach revealed that the distal pressure line connection (labeled with blue coloring) had become loose presumably from the patient holding the device with her hand during testing.
With a pressure differential pneumotach any leak in the distal pressure line will falsely elevate the gradient across the metal screen resulting in spuriously high flows and volumes.

Figure 5. A loose distal pressure line (labeled blue).
Repeat post bronchodilator testing after re-insertion of the distal pressure line demonstrated the true bronchodilator response.
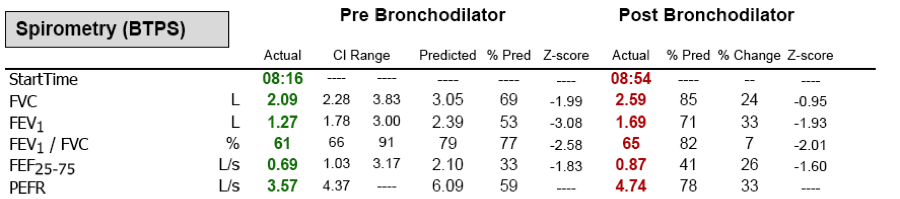
Figure 6. Pre and post-bronchodilator data following re-insertion of the distal pressure line.
Teaching points:
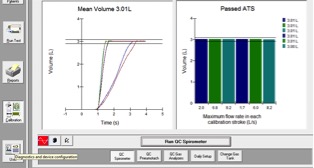
- Pre-test quality control testing is essential to quality pulmonary diagnostics; however, technologists must be mindful that equipment function can change during testing.
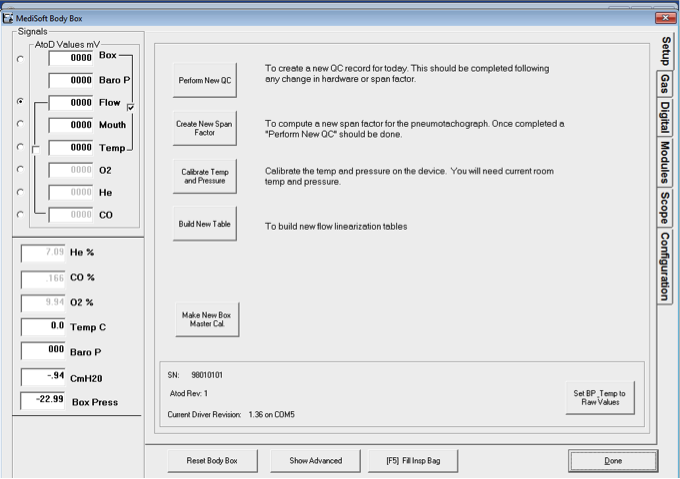
- If measured values seem out-of-place, re-calibration should be performed. To perform a new calibration in ComPAS go to diagnostics and select “perform new QC”
- Understanding exactly how your equipment measures pulmonary function is essential for timely and correct troubleshooting.